Overview
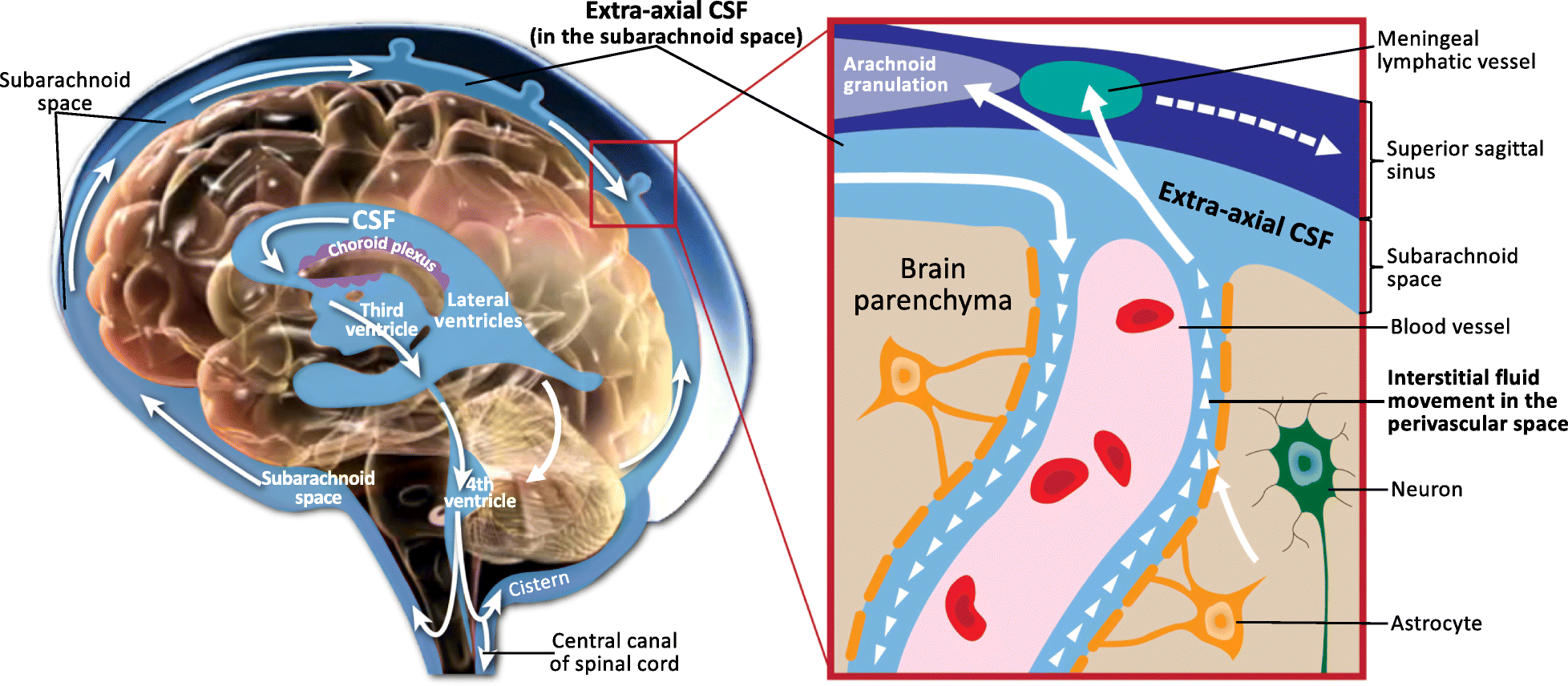
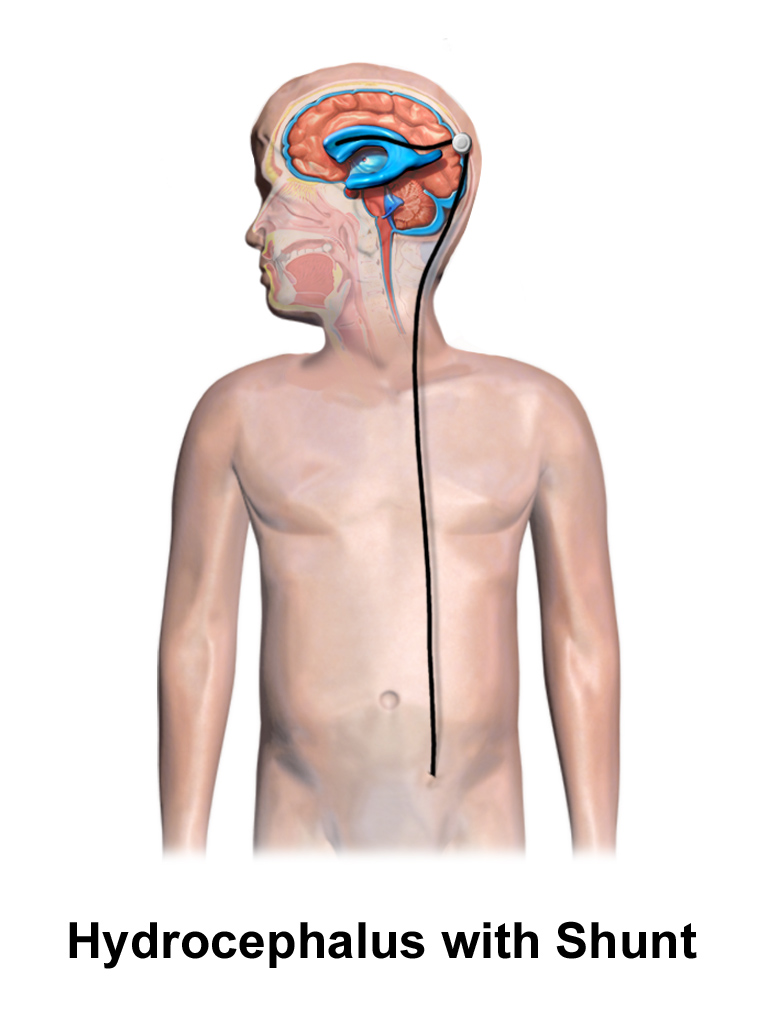
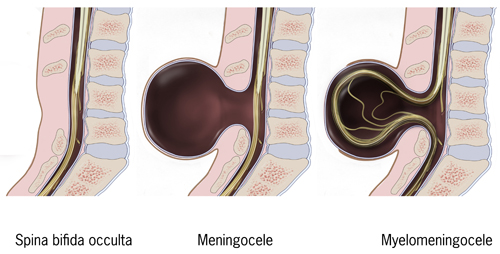
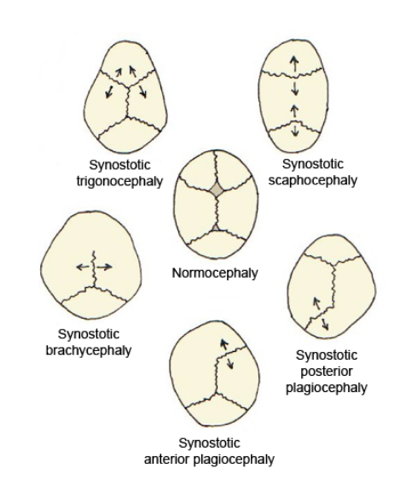
This module covers the principal CSF disorders and congenital malformations of the central nervous system encountered in paediatric neurosurgery. Hydrocephalus is the most common neurosurgical condition of childhood, with a wide spectrum of aetiologies (congenital aqueductal stenosis, post-haemorrhagic dilatation of prematurity, post-infectious, tumour-related, and post-traumatic). Congenital malformations span open neural tube defects (now reshaped by the MOMS-era of in-utero repair), Chiari malformations, encephaloceles, the Dandy-Walker spectrum, the craniosynostoses, and the closed spinal dysraphisms (lipomyelomeningocele, dermal sinus tract, split-cord malformations, and tethered cord).
Modern paediatric hydrocephalus practice is defined by two intertwined choices: shunt versus endoscopic third ventriculostomy (ETV), with or without choroid plexus cauterization (CPC). Selection is increasingly evidence-informed using the ETV Success Score (Kulkarni et al., 2010) and accumulated multi-centre data from the Hydrocephalus Clinical Research Network (HCRN). Congenital malformation care is multidisciplinary by necessity, with prenatal diagnosis and counselling now routine in most regions.
References used here
-
Albright AL, Pollack IF, Adelson PD. Principles and Practice of Pediatric Neurosurgery. 3rd Edition. Thieme, 2015. ISBN: 978-1-60406-799-6.
-
Winn HR (Editor). Youmans and Winn Neurological Surgery. 8th Edition (4-volume set). Elsevier, 2022. ISBN: 978-0-323-66192-8.
-
Greenberg MS. Greenberg's Handbook of Neurosurgery. 10th Edition. Thieme, 2023. ISBN: 978-1-68420-504-2.
-
Kulkarni AV, Drake JM, Kestle JR, Mallucci CL, Sgouros S, Constantini S. Predicting who will benefit from endoscopic third ventriculostomy compared with shunt insertion in childhood hydrocephalus using the ETV Success Score. J Neurosurg Pediatr. 2010;6(4):310-315.
-
Adzick NS, Thom EA, Spong CY, Brock JW 3rd, Burrows PK, Johnson MP, Howell LJ, Farrell JA, Dabrowiak ME, Sutton LN, Gupta N, Tulipan NB, D'Alton ME, Farmer DL. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011;364(11):993-1004.